Radiation Dose Units in Radiological Protection
This post is written assuming a foundational knowledge of the different types of radiation. For more information, please see our free course, Understanding Radiation.
When we look at a system of units, you have things that are being measured and units used to report them. For example, the quantity speed is the rate at which distance is being covered. It can be reported in the units of kilometers per hour, meters per second, miles per hour, etc. Sometimes a combination of units is used so frequently that it is given its own name. For example, a nautical mile per hour is called a knot. These are often given short forms.
There is also typically a letter assigned to a quantity when using it in a formula. (They do not always match the first letter of the quantity.) To summarize our examples:
| Quantity | Formula Letter | Unit | Unit Short Form |
| speed | v | kilometers per hour | km/h |
| meters per second | m/s | ||
| miles per hour | mph | ||
| knots | kn or kt |
Units Systems Used in Radiological Protection
You may remember from school being taught that matter has mass and takes up space. And energy is the ability to change matter in specific ways. Radiation is energy travelling out from a source. When it interacts with matter, it can deposit some or all of its energy into the material.
When it comes to radiological protection, we need to be able to discuss not only how much energy has been deposited into human tissue as a result of radiation exposure, but also the biological consequences of this energy. There are two main systems of quantities and units used for this purpose. One is part of the International System of Units (SI), which is what is mainly used in Canada. The other is a traditional system based on CGS (centimeters, grams, seconds) that is still used in the United States and in some industries or situations. This post will focus on SI units.
Under the SI system, the International Commission on Radiation Units and Measurements (ICRU) Report 85a: Fundamental Quantities and Units for Ionizing Radiation (Revised) is the foundational reference document on the topic.
Tissue Reactions vs Stochastic Effects
When radiation deposits energy into our tissues, any resulting health effect can manifest in one of two ways: tissue reactions (previously called deterministic effects) and stochastic effects. To understand the difference, consider the incidence of the health effect as the cause of the effect is increased from low levels.
If the effect does not appear until a threshold is reached, and then gets worse the more energy is deposited, it is a tissue reaction. (The threshold can be different for each individual.) Examples include radiation burns, cataracts, and acute radiation syndrome. What is occurring at the cellular level is that many cells are killed off or modified in a way that impairs the function of the tissue of which they are part.
If the effect is not guaranteed to occur over a threshold, but rather the incidence in a population who are exposed is greater than in an unexposed population, and the risk gets higher as the doses received within that population get higher, it is a stochastic effect. These effects are due to damage to DNA and other molecules involved in life processes that goes unrepaired or is incorrectly repaired. Cancer in humans is a stochastic effect.
On this topic, in Report 85a, the ICRU states, “On a practical level, this Report adopts the convention that a quantity whose underlying distribution at microscopic levels is normally of little interest and that is customarily expressed in terms of a mean value will not be defined explicitly as stochastic.” In other words, quantities where the average energy deposited determines the occurrence and severity of the health effect rather than the precise distribution of the energy at the molecular level are considered non-stochastic.
Absorbed Dose
The amount of energy that is absorbed per unit mass of material by ionizing radiation is called absorbed dose. In the SI system, the standard unit for energy is the joule (J) and for mass, the kilogram (kg). So absorbed dose as a quantity is reported in units of J/kg. But this is one of the cases where a combination of units is given a name: the gray (Gy).
1 J/kg = 1 Gy
The letter used for absorbed dose in a formula is D.
Kerma
Charged-particle radiation, including alpha and beta, can strip electrons off of atoms or molecules without touching through the interaction of electric fields. Gamma, x-ray, and neutron radiation do not have charge and therefore must directly interact with or hit a piece of material in the atom in order to be able to ionize. The ejected charged particles then go on to ionize more atoms than that single one. For this reason, they are called indirectly ionizing.
For indirectly ionizing radiation, there is another quantity that is sometimes used: kerma. This stands for Kinetic Energy Released in Matter. This quantity is a measure of the initial kinetic energy of the charged particles the indirectly ionizing radiation caused to be released per a set unit of mass. Because it is still energy per unit mass, in the SI system its unit is still the gray and in the traditional system, the rad.
This may seem like an unnecessary distinction. But to use a financial analogy, if you only know your gross income for a month, you do not know details of the impact of the money. However, if you examine specific uses of your funds, you can understand how that money has impacted your financial status in particular ways. For example, was it used to pay down debt, put in a tax-free savings account, invested in your RESP, left sitting in a low-interest account, etc.?
When radiation interacts with material, it can do other things besides ionize. It may heat the material, cause electrons to become excited but not totally remove them from an atom, or cause a chemical reaction that wouldn’t otherwise happen (photochemical effect), amongst other things. Because it is the ejected charged particles that go on to ionize further, by considering only their energy instead of the total energy absorbed, you can focus on the ionizing effect of that radiation. For photons at low energies, in the ranges commonly used in diagnostic and industrial radiography, absorbed dose and air kerma will be similar in value for a given radiation exposure.
Equivalent Dose
Different types of ionizing radiation deposit their energy into tissue in different ways. This changes the risk of getting stochastic effects like cancer, even if the absorbed dose is the same. To account for this, the International Commission on Radiological Protection (ICRP) refers to a quantity called equivalent dose. It represents the relative biological risk of a tissue or organ receiving an absorbed dose of radiation using gamma radiation as the standard. Its unit is the sievert (Sv) and it is given the letters HT in a formula.
By examining a large body of scientific studies, the ICRP has recommended radiation weighting factors to convert absorbed dose to equivalent dose. The weighting factors have no units and are given the symbol wR in a formula. To calculate equivalent dose to a tissue from a single type of radiation, you multiply the absorbed dose by the appropriate radiation weighting factor and switch the unit from Gy to Sv
From ICRP 103, “The unit of equivalent dose is J kg-1 with the special name sievert (Sv).”
The radiation weighting factors recommended in ICRP 103, their most recent as of the date of this post, are:
| Radiation Type | Radiation Weighting Factor |
| Photons (gamma, x-ray) | 1 |
| Electrons and muons | 1 |
| Protons and charged pions | 2 |
| Alpha particles, fission fragments, heavy ions | 20 |
| Neutrons | A continuous function of neutron energy |
If a tissue is exposed to several different types of radiation, to find the total equivalent dose to that tissue, you account for each radiation dose separately using the weighting factor and add the equivalent doses together.

Effective Dose
Different tissues in the human body have different sensitivity to being exposed to ionizing radiation. Similar to equivalent dose, the ICRP uses a quantity so that we might compare the relative risk from an absorbed dose received by a given tissue or organ to a whole-body dose of gamma radiation. This is named effective dose. The unit is still the sievert because this quantity also represents relative biological harm as it relates to stochastic effects. It is given the letter E in a formula.
The ICRP has recommended tissue weighting factors used to make this comparison. The weighting factors have no units and are given the symbol wT in a formula. From ICRP 103, “These wT values are chosen to represent the contributions of individual organs and tissues to overall radiation detriment from stochastic effects.”
For a single tissue, starting from equivalent dose to convert to effective dose, you multiply by the tissue weighting factor.
The tissue weighting factors recommended in ICRP 103, their most recent as of the date of this post, are:
| Tissue Type | Tissue Weighting Factor |
| Bone-marrow (red), Colon, Lung, Stomach, Breast, Remainder tissues* | 0.12 |
| Gonads | 0.08 |
| Bladder, Oesophagus, Liver, Thyroid | 0.04 |
| Bone surface, Brain, Salivary glands, Skin | 0.01 |
| *Remainder tissues: Adrenals, Extrathoracic (ET) region, Gall bladder, Heart, Kidneys, Lymphatic nodes, Muscle, Oral mucosa, Pancreas, Prostate, Small intestine, Spleen, Thymus, Uterus/cervix | |
If there are a number of different tissues that must be considered, each equivalent dose is multiplied by its tissue weighting factor and then the individual effective doses are added.

Or if beginning from absorbed dose, you have to multiply each absorbed dose by its radiation weighting factor and its tissue weighting factor, and then add them.
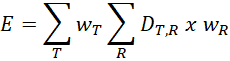
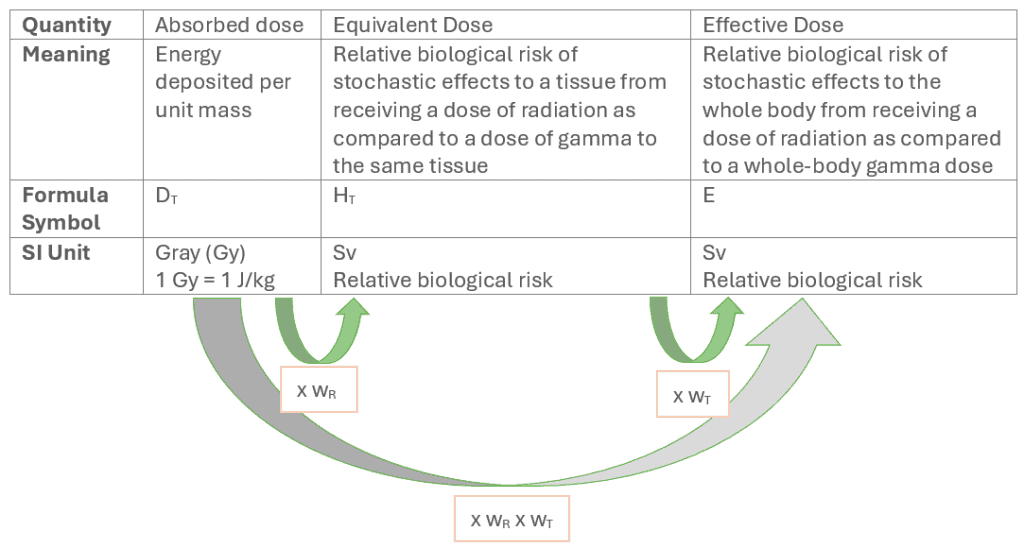
To summarize the relationship between absorbed dose, equivalent dose, and effective dose:
When to Use Which
When teaching radiation protection, we often get the question of why doses related to some biological effects are reported in gray when workers are more familiar with the sievert. For example, thresholds for tissue reactions are reported in gray while dosimetry reports and equivalent and effective dose limits are reported in sieverts.
Going back to the discussion of tissue reactions vs stochastic effects, we have units that correspond to each. The gray is the unit for a physical quantity. It is used to report the amount of energy absorbed into a tissue. For effects that are not dependent on the probabilistic nature of damage, such as the energy killing a cell outright or causing a chemical reaction that impairs function like the formation of cataracts, it is the best unit to report dose. In other words, if discussing tissue reactions/deterministic effects, the unit to be used is the gray.
The sievert is a unit derived from epidemiological and radiobiological data. It is used when relative biological risks of stochastic effects are being discussed. In these cases, the precise nature of the damage to molecules related to life and the individual’s body’s response to that damage determines the outcome over time.
Equivalent and effective dose are what are known as protection quantities. ICRP 103 gives the detail on their purpose: “[t]he protection quantities are used to specify exposure limits to ensure that the occurrence of stochastic health effects is kept below unacceptable levels and that tissue reactions are avoided.”
These protection quantities were developed with weighting factors based on stochastic effects. Equivalent dose limits are based on preventing tissue reactions, but are reported in sievert. Most workers will not encounter the use of the gray in their dosimetry reports or dose estimates. But the gray is foundational to the meaning of the sievert and used to report thresholds for tissue reactions.
No wonder people get confused.
This overlap of the two units is addressed in ICRP Publication 147: Use of Dose Quantities in Radiological Protection, where the ICRP states:
Absorbed dose is the most appropriate quantity for use in setting limits on organ/tissue doses to prevent tissue reactions (deterministic effects). Equivalent dose is an intermediate quantity in the calculation of effective dose, and the radiation weighting factors (wR) applied to absorbed doses and used in the calculation of equivalent dose relate to stochastic effects at low levels of exposure rather than tissue reactions. The Commission considers that the use of equivalent dose to set limits on organ/tissue doses to prevent tissue reactions should be discontinued, but that current limits can continue to be applied until new general recommendations are issued. Radiation weighting for tissue reactions will require further consideration.
Equivalent dose and effective dose are not measurable in practice. Operational quantities such as Hp(10) and Hp(0.07) are used to assess effective dose or equivalent dose in practice. We will cover these in a future blog post.
This post only touches the surface of the Recommendations of the ICRP and related material. For full details, please refer to their publications: https://www.icrp.org/page.asp?id=5.